Total Hip Replacement – Post-op Instructions
Guidelines after Total Hip Replacement surgery
Congratulations on your new Total Hip Replacement (THR)! I am excited to guide you through your recovery as you begin to regain your active lifestyle. This document will attempt to help you through your recuperation with activity guidelines, as well as answer some of the most common questions that patients have after undergoing this procedure.
By the time you have left the hospital/rehab facility, you should be able to get in-out of bed by yourself, walk with the cane several hundred feet, and go up and down stairs. The biggest challenge in the early recovery of a THR (up to 6 weeks postoperative) is maintain your hip precautions to prevent dislocation.
We will send a physical therapist to your house to help you with the walking and hip exercises. The therapist will likely come to your residence 2 to 3 times per week. On the days that the therapist does not come, it is still important for you to continue walking and perform your exercises. Most patients will continue to need the cane for walking until 2-4 weeks postoperative; if you feel that you still need it for safety/balance, please continue to use it.
I like to see you in the office and examine you before prescribing outpatient physical therapy. If your home therapist feels that you are finished with the home regimen and stops going to your house, please wait until you return to my office before going to outpatient PT.
Walking:
I recommend that you walk as much as your feel comfortable (at least 2-3 times a day), trying to walk a little further each time. You may walk inside or outside as you feel comfortable. As stated above, you will need a walker or cane for stability for the first 3-6 weeks. When you begin to felt that you don’t need the cane anymore, you can begin to wean from the cane; that is, you can stop using it for short distances and walk further and further without it. Pretty soon you will be forgetting to use your cane!
Motion:
You need to maintain hip precautions in order to avoid dislocation. These precautions include: not bending at the hip more than 90 degrees, sleeping with a pillow between your legs, not turning the toes inward, not pivoting at the hip, and not crossing your legs. To maintain these restrictions, you will have to sit on high chairs (or with a cushion), use a high toilet seat, and use reacher/sock-aids. You must maintain these precautions until I see you in the office.
Pain control:
Once you get home and further out from surgery, you may try to wean from the pain medication, as there are many side effects of taking narcotics. I suggest that you try decreasing the amount of pain medication or increasing the interval between doses in order to wean from the medication during the day. You may have to try different methods to see what works best for you. You can also take an anti-inflammatory medication such as ibuprofen (Advil) or naproxen (Aleve), if your stomach can handle this.
Exercises:
The early exercises for the THR consist of the following, and should be done by performing 5 sets of 10 through the course of the day:
- Ankle pumps
- Quad sets (pressing the knee down)
- Gluteal squeezes
Later exercises should be done in the same fashion and include:
- Side raises (abduction) in a standing position and while lying on your side
- Hip extensions (moving the hip backwards) in a standing position
- Limited straight leg raises (do not do this with any weights)
I recommend that you walk as much as your feel comfortable (at least 2-3 times a day), trying to walk a little further each time. You may walk inside or outside as you feel comfortable. As a rough guideline, patients can walk up to 1 mile at a time, by 2 weeks after surgery. My best advice to you during your recovery is to listen to your body – that is, if you feel pain during an exercise or afterwards, you have probably overdone it
Please call my office to make a followup appointment at 6 weeks post-operative to see one of my physician assistants. We will obtain x-rays of your new hip and go over the plan to continue making progress.
Instructions after first postop visit (6-8 weeks after surgery):
You should now be comfortable in walking with a cane or nothing at all, placing full weight on the operated leg. At this point, if you haven’t already done so, you may wean to using 1 crutch or cane in the opposite hand/arm. I like to think about your rehabilitation in 3 phases:
- Phase I (day 1 to 1 month postop) – acute post-operative; mainly concentrating on walking correctly and doing some simple exercises.
- Phase II (1 month to 4 months postop) – stretching exercises to regain hip flexibility and range of motion, gentle strengthening
- Phase III (3 months to 1 year postop) – strengthening exercises.
Note: there is some overlap between the phases, and patients will feel ready for the next phase at different timepoints. The timings are only rough guidelines for your reference.
After surgery, you will experience the formation of scar tissue. This scar tissue will form not only at the incision site, but also deep within the joint. It is common at this point to still have a feeling of stiffness, particularly if you have stayed in one position for too long. I recommend changing position every 1-2 hours to avoid this feeling.
During Phase II, the goal is to stretch out this scar tissue while it is still pliable. You will continue to gain motion for up to a year, but it is easier the earlier we start. I recommend doing the following exercises daily, 3 to 4 times per day. In addition, I will prescribe outpatient therapy to have a physical therapist assist with the strengthening aspect.
These 2 exercises should be done on your own to increase flexibility:
- “Dangle”: This is a simple exercise to help increase flexion.
Just find a stool or lower chair. Place your knees at shoulder width. Bring your hands down towards your ankles and hold when you feel the stretch. Don’t bounce or continue if you have a lot of pain. Repeat for a set of 10.

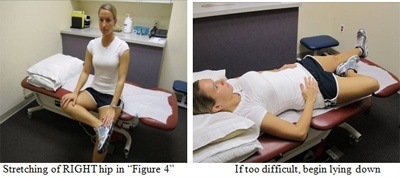
- “Figure 4 crossing of legs” : This exercise is designed to increase the rotation in your hip joint, particularly so that you can put on your own shoes and socks.
In a sitting position, gently grab your operated foot and bring it to rest on your unoperated knee. This will bring you into a sitting, cross-legged position. It will be difficult at first, and you may feel some pain around the incision site. If it is too stiff to accomplish this early on, you may turn your body at an angle to the chair/bed, and bring the foot onto the chair/bed instead of your opposite knee. Gently press on your operated leg to flatten it.
In addition to these exercise and your physical therapy, you can continue to increase your activity. I still recommend swimming the breaststroke, riding a bicycle, and walking. As you become confident in cycling, you can venture onto the road, as long as you don’t fall.
You can use an elliptical machine when you no longer use a cane or crutch.
In terms of strengthening exercises, I recommend particularly the exercise of side-raises (abduction). This will stabilize your pelvis and eliminate a limp.
In the beginning, you will not have the strength to lift the leg unsupported, so I recommend starting with “clamshell” exercises:
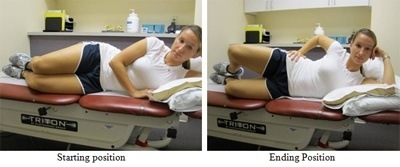
Advanced abduction exercises (with operated leg unsupported):
To do this properly, you should lie on your unoperated side. Place your operative leg slightly behind your torso (in extension) and raise slowly. You can do this while lying against a wall, placing light pressure of your operated heel against the wall to ensure you are doing it correctly.
WARNING
An artificial hip joint is never as stable as your own hip joint. Therefore, there are some movements that are prohibited with a THR, so that you don’t dislocate the hip joint. If you dislocate your hip joint, you will feel extreme pain and have to go to an emergency room to have the hip put back into place.
You should always remember that an artificial hip is always SAFEST with your legs apart. Try to keep your knees shoulder-width apart when you are sitting. You should AVOID bringing the knee on the operated side to your shoulder, as this is too steep an angle. You should keep the space of about 6 inches between your knee and shoulder if you are bringing your knees toward your chest.
You should also avoid internal rotation of your hip. This means that you would twist the knee of your operated leg inward. Beware of this motion when you are trying to get to your feet; some women will do this when shaving the outside of their legs – avoid this! Also, do not twist toward the operated side when you are sitting, as this will cause internal rotation of the hip.
In the next few months, you can gradually return to sports. Remember to listen to your body. You can begin swinging a golf club or tennis racquet at about 3 months after surgery. With golf, you should work on your short game first. With tennis, you should hit ground strokes in place before chasing down balls. An improved range of motion will help with both of these sports. After completing outpatient PT, you can do some yoga to continue with stretching, if desired.
I would like you to be comfortable putting on your shoes and socks by 3 months postoperative. Remember that stretching is a dynamic process and will continue to improve. Otherwise, you are free to enjoy your new hip!
For frequently asked questions please click here.



